Advanced practitioner physiotherapists Krystian Dawiec and Tom Causebrook discuss recent developments in the management of osteoarthritis in primary care
Module summary
NICE guidelines on osteoarthritis now place an emphasis on exercise in its management. In practice, the pain and mobility problems faced by patients with osteoarthritis can make regular exercise a challenge.
Here primary care physiotherapists Krystian Dawiec and Tom Causebrook explain how exercise can help in managing osteoarthritis and how it can be safely and effectively implemented. They also discuss the role of other interventions in osteoarthritis management and what pharmacological options are now recommended.
Learning objectives:
- Understand the management options in osteoarthritis, including the central role of exercise
- Be able to confidently advise patients on how exercise can help manage pain and improve mobility
- Gain an understanding of the key pharmacological adjuncts
- Appreciate the role of psychological support and weight loss
- Recognise when surgery is appropriate and how this is accessed
Definition of osteoarthritis and diagnostic criteria
Osteoarthritis (OA) has historically been considered as ‘wear and tear’ in the human synovial joints.
In reality, age is only one of many factors that may predispose us to the disease, alongside overuse, past trauma or injury, genetics or family history, occupation, gender and obesity. The condition is indeed multifaceted, with both mechanical and inflammatory components leading to joint damage.
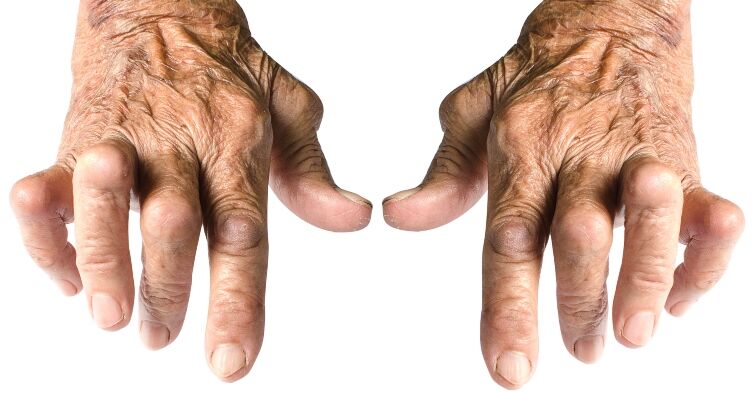
Given the aforementioned factors, OA commonly affects the weight bearing joints of the hips and knees, but is not exclusive to the lower limb – the basal thumb joint, distal interphalangeal hand joints and lumbar and cervical spine are also commonly affected.
OA often causes joint pain and stiffness that worsens with activity and at the end of the day, and can often result in joints becoming swollen. Resting and offloading the irritable joint will usually ease symptoms. This presentation is the opposite to the pattern seen in inflammatory arthritis, where symptoms are worse in the morning and typically improve with activity.
Clinicians should be aware that any joint swelling associated with systemic symptoms (high temperature, malaise, confusion and inability to weight bear due to severe pain) should prompt emergency investigation to rule out the diagnosis of septic arthritis. A history of recent trauma and inability to weight bear, immediate joint effusion or joint deformity should alert clinicians to the possibility of fracture.
Mild to moderate OA can cause bony enlargement around the joints, reduced joint mobility, crepitus (clicking, cracking or popping noises) during joint movement and swelling due to fluid building up around the joint after overuse.1 In more severe or chronic OA cases, joint deformity, increased stiffness and sometimes instability of the joint can be present.
The NICE guidelines advise that a diagnosis can be made without any investigations if the patient is over 45 and has typical pain associated with activity and no morning stiffness (or stiffness lasting under 30 minutes), has symptoms that have been present for over 3 months and for whom an alternative diagnosis is unlikely.2,3
Conservative management of OA – the central role of exercise
Regular exercise has multiple health benefits. However, for people with OA, performing regular exercises can be difficult due to pain and limited mobility.4 Nevertheless, based on substantial evidence from clinical research, NICE recommends that exercise should take a central position in the overall management of OA, rather than pain relief prescription and surgical intervention.2,5
Exercise increases muscle strength, improving the stability of the joints affected by OA. This results in improved joint resilience to cope with everyday load. Exercise also improves joint mobility and prevents further mobility deterioration. Furthermore, during exercise mental health and pain levels improve, due to the release of endorphins, increased tissue oxygenation and clearance of metabolic substance which can have proinflammatory properties. Patients whose muscles are adequately strong tend to recover a lot more quickly from joint replacements and have lower complication rates.
Exercise should be individually tailored to optimise the health benefits in patients with OA. The NICE guidance provides some detail in terms of what exercises should be advised to patients in an attempt to standardise and improve care across the UK, recommending that both local muscle strengthening and generalised aerobic fitness exercises are beneficial.2
To complete the full module visit the Nursing in Practice 365 website.
Not a Nursing in Practice 365 subscriber? Register for free or gain access to more CPD content as a Premium member.
Krystian Dawiec is an advanced clinical practitioner and musculoskeletal clinical lead based in primary care and is also a consultant physiotherapist in private practice.
Tom Causebrook is an advanced physiotherapy practitioner splitting his time between first contact physiotherapy clinics in primary care and orthopaedic interface services, as well as managing a busy sports and orthopaedic clinic.